What is biocompatibility? Everyone has a vague idea of what the term means but you will never get a clear precise definition of biocompatibility. The FDA defines biocompatibility as:
“The ability of a device material to perform with an appropriate host response in a specific situation.”
The FDA has recently made clearance for medical devices much more stringent with a much more expanded array of biocompatibility tests needed for market clearance.
Nearly all current bone graft products on the market, including SteinerBio products, have never been subjected to this new level of testing. Many drugs, including many bone graft products, have significant side effects. The FDA accepts a certain level of side effects and often accepts very significant side effects when it approves medications and medical devices. However, products that are designed for regenerative medicine are unique from all other products because excellent biocompatibility is required for normal tissue regeneration.
For the body to regenerate itself, it must duplicate the biological processes that formed the tissue in the first place and inflammation is never a component of normal tissue growth. If a drug or device produces any inflammation, you will not produce normal healthy tissue. While inflammation is a blocker for tissue regeneration, the concept of biocompatibility encompasses an even greater array of biological processes other than just the inflammatory response.
The FDA’s Good Laboratory Practices (GLP) provide regulations by which safety studies are conducted. GLP testing is far more complex than research publications. Extensive protocols are produced that must be in accordance with FDA standards. When producing the protocols, a team of quality control personnel must be employed to ensure the study design is appropriate and followed precisely. Every team member involved in the study must have GLP training by certified bodies. The protocols, documentation, and reports are complex and extensive. The reason for this research complexity is that it makes it possible for the FDA to reproduce the study exactly if it questions the results.
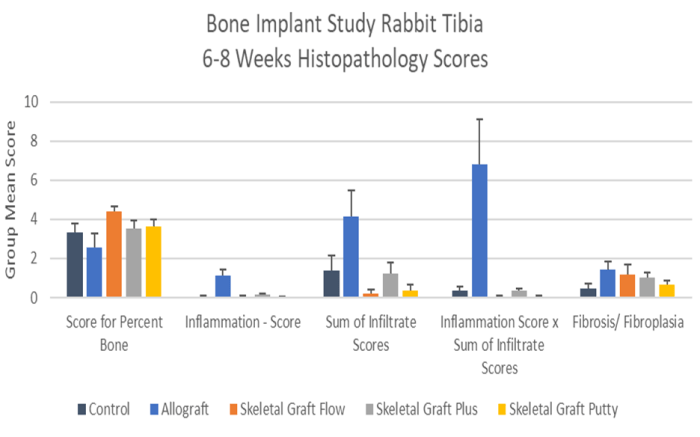
SteinerBio is taking its regenerative technology to the skeleton. For our submission to gain clearance for use in the skeleton, we have completed five different studies. Four of the five studies were performed by a specialized testing facility completely independent of SteinerBio. The fifth study was a bone graft study on rabbits. For this study, the FDA spent a week in our facility to review the documentation and approved the protocol. The tissue samples were produced by SteinerBio, but the analysis was performed by an independent testing facility. The tests performed on SteinerBio products for the evaluation of biocompatibility are as follows: