Ridge Augmentation and the Etiologyof Buccal Alveolar Resorption
The following ridge augmentation case is interesting in its own light, but what is more interesting is what it can teach us about bone resorption. We will discuss why buccal resorption occurs and propose treatment that might limit the loss of buccal bone after tooth extraction.
Planned ridge augmentation and extraction.
Buccal and lingual loss of alveolar ridge.
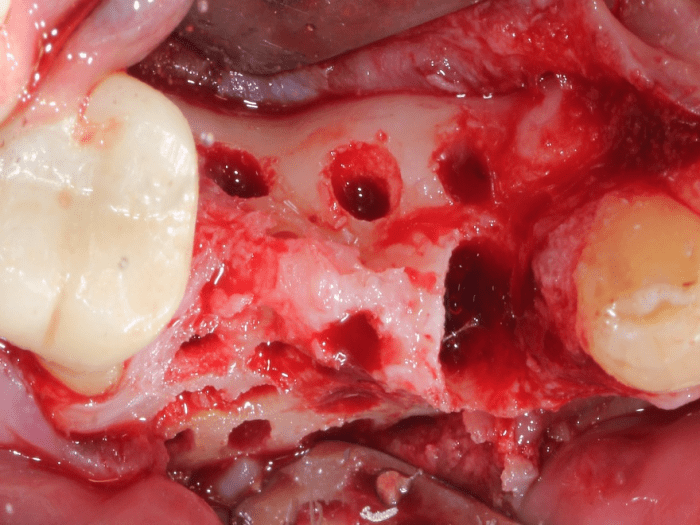
Cortical bone perforated to access regenerative cells.
Grafted with Ridge Graft Kit, which is our βTCP granules mixed with our regenerative putty.
D-PTFE membrane with no tacks.
The membrane exposed and was removed after one month.
4.5 months after grafting.
The coronal cortical perforations are fading as they are covered with new alveolar bone. The apical cortical perforations are prominent as a result of being apical to the graft site.
4.5 months post graft, area of bicuspid.
The lingual crest shows a lower density distinguishing newly formed cortical bone at the crest from preexisting lingual cortical bone.
4.5 months post graft, area of core sample.
4.5 months post graft, area adjacent to distal molar.
5.5 months after grafting.
The majority of the lingual graft material is resorbed and converted into new cortical bone. The buccal graft site is still covered with a thin layer of graft material. To better understand the regenerative process a core sample was taken buccal to the distal implant.
Shallow core sample.
The surface of the alveolus shows OsseoConduct™ βTCP granules encased in woven bone. The granules were only approximately 1 mm deep into the core sample.
A high power of a βTCP granule covered in woven bone.
Under the surface of woven bone and βTCP granules, the core sample is composed of lamellar cortical bone. All graft material has been resorbed.
Medium power of the previous slide showing lamellar cortical bone. While the core sample shows lamellar bone, the lamellar bone is not aligned along any organized pattern. The reason for this lack of organization is because this area is not under load. When load is applied with the function of an implant, reorganization of the bone will occur into a pattern aligned to carry the load being applied.
A high power of the newly formed lamellar cortical bone.
An interesting note is the rapid pace of lingual bone formation when compared to the buccal bone formation. On the lingual, the cortical bone is much more mature and the resorption of the granules is nearly complete. On the buccal, the conversion from bone graft material to cortical bone is not as complete.
The CT scan from the area of the core sample shows the lingual cortical bone completely regenerated at 4.5 months, but the buccal cortical bone is still maturing, even though the core sample shows newly formed lamellar bone.
Bone regeneration is always interesting and this case is no different. Here, we have a chance to compare buccal and lingual bone regeneration and we find that lingual bone formation proceeded much quicker than buccal bone formation. When no load is present, it appears that our bodies aggressively regenerate lingual bone but buccal bone regenerates more passively.
It is proposed that buccal bone and lingual bone have two different purposes. Because a tooth is floating in a periodontal ligament, the tooth does not contribute to the load carrying mass of the jaw. It is proposed that the purpose of the buccal bone is to support the tooth and the purpose of the lingual bone is to support the load carrying capacity of the jaw. When a tooth is removed, there is no need for the buccal bone, therefore, it is resorbed. However, if the purpose of the lingual bone is to support the load carrying capacity of the jaw to prevent fracture, the lingual bone is maintained.
This is a radiograph of the molar immediately distal to the distal implant. As is obvious in this radiograph, the amount of lingual bone far exceeds the amount of buccal bone. The buccal bone is necessary to support the tooth, but contributes very little to the support of the load carrying capacity of the jaw. When the tooth is removed, the buccal bone becomes superfluous and subject to resorption while the lingual bone is maintained because it is required for the load carrying capacity of the jaw.
It needs to be mentioned that none of these regenerative principals will apply to cadaver bone grafts. Cadaver bone grafts form sclerotic bone that never transition into cortical or cancellous bone. You will never see cortical bone clinically or histologically in a site grafted with cadaver bone grafts. You can prove this to yourself if you look at CT scans of ridge augmentation sites grafted with cadaver bone grafts and you will only see a homogeneous mass, no matter if it is 6 months or 6 years. Want to prove us wrong? You can send clinical photos, histology, or a CT scan showing a cadaver graft site that has formed cortical and cancellous bone and we will publish it to all of our audience.
MEMBER:
American Society for Bone and Mineral Research (ASBMR)
Tissue Engineering and Regenerative Medicine International Society (TERMIS)